
When we picture dementia, most of us picture forgetting: a parent who mislays their keys, repeats a question, or can’t recall a grandchild’s name. That image is so fixed that when the first symptom is something else entirely, a warm, generous person turning cold, a careful spender making reckless decisions, a devoted partner losing all interest in the people they love, families rarely think “dementia” at all. They think about stress. Burnout. Depression. A difficult phase. A midlife crisis.
This is the quiet tragedy of frontotemporal dementia (FTD). It often begins not with a failing memory but with a changing personality, and because that doesn’t match what we expect, it is one of the most under-recognised and frequently misdiagnosed forms of dementia there is. At Kuremara, our home care teams across the UK regularly support families who have spent years searching for an explanation before anyone said the word “dementia” out loud. This article is written to shorten that search for others to explain what FTD is, why it hides in plain sight, and what to do if the changes you’re seeing in someone you love don’t fit the usual story.
What Frontotemporal Dementia Actually Is
Frontotemporal dementia is an umbrella term for a group of conditions caused by damage to the frontal and temporal lobes, the regions at the front and sides of the brain that govern personality, behaviour, emotional control, decision-making, and language. As nerve cells in these areas are damaged and die, the brain tissue there gradually shrinks, and the abilities those regions control begin to slip away.
Crucially, memory is often not the first thing to go. As the NHS explains, in FTD, memory problems tend to occur only later on, unlike more common forms of dementia such as Alzheimer’s disease. That single difference is why so many families are caught off guard. The part of the brain that remembers where you put your glasses can be working almost normally while the part that governs empathy, judgement, and social behaviour is quietly failing.
FTD is also, in one important respect, unlike the dementia most people have in mind: it strikes younger. It is most often diagnosed in people in their 40s, 50s and 60s, according to the UK Dementia Research Institute, an age when someone may still be working, raising children, paying a mortgage, and at the very centre of family life. When a person of that age begins to change, dementia is rarely the first explanation anyone reaches for, including their doctor.
Why It’s Less Rare Than It Feels
FTD is genuinely less common than Alzheimer’s disease. The Alzheimer’s Society notes that around 1 in 20 people living with dementia in the UK have a rarer type, and FTD sits within that group. But “less common” is not the same as “rare in the group that matters.” Among people who develop dementia before the age of 65, so-called young-onset dementia, FTD is one of the leading causes, second only to Alzheimer’s disease.
The numbers bear this out. Population studies in the UK have estimated a prevalence of roughly 15 cases per 100,000 people aged 45 to 64. To put that in human terms: FTD is not a medical curiosity confined to textbooks. It is an ordinary tragedy that unfolds in ordinary households, most often in people who are still in the prime of their working and family lives, and it is very likely more common than official figures suggest, because it is so frequently mistaken for something else.
The Two Faces of FTD: Behaviour and Language
FTD doesn’t look the same in everyone. Its symptoms depend entirely on which parts of the frontal and temporal lobes are affected first, and clinicians generally recognise a few distinct patterns.
1. Behavioural variant FTD
This is the most common form, and the one most likely to be misread as a psychological problem rather than a physical illness of the brain. When the parts of the frontal lobe that control social behaviour are damaged, the changes are unsettling precisely because they alter who a person seems to be. Drawing on descriptions from the NHS and Alzheimer’s Research UK, the early signs can include:
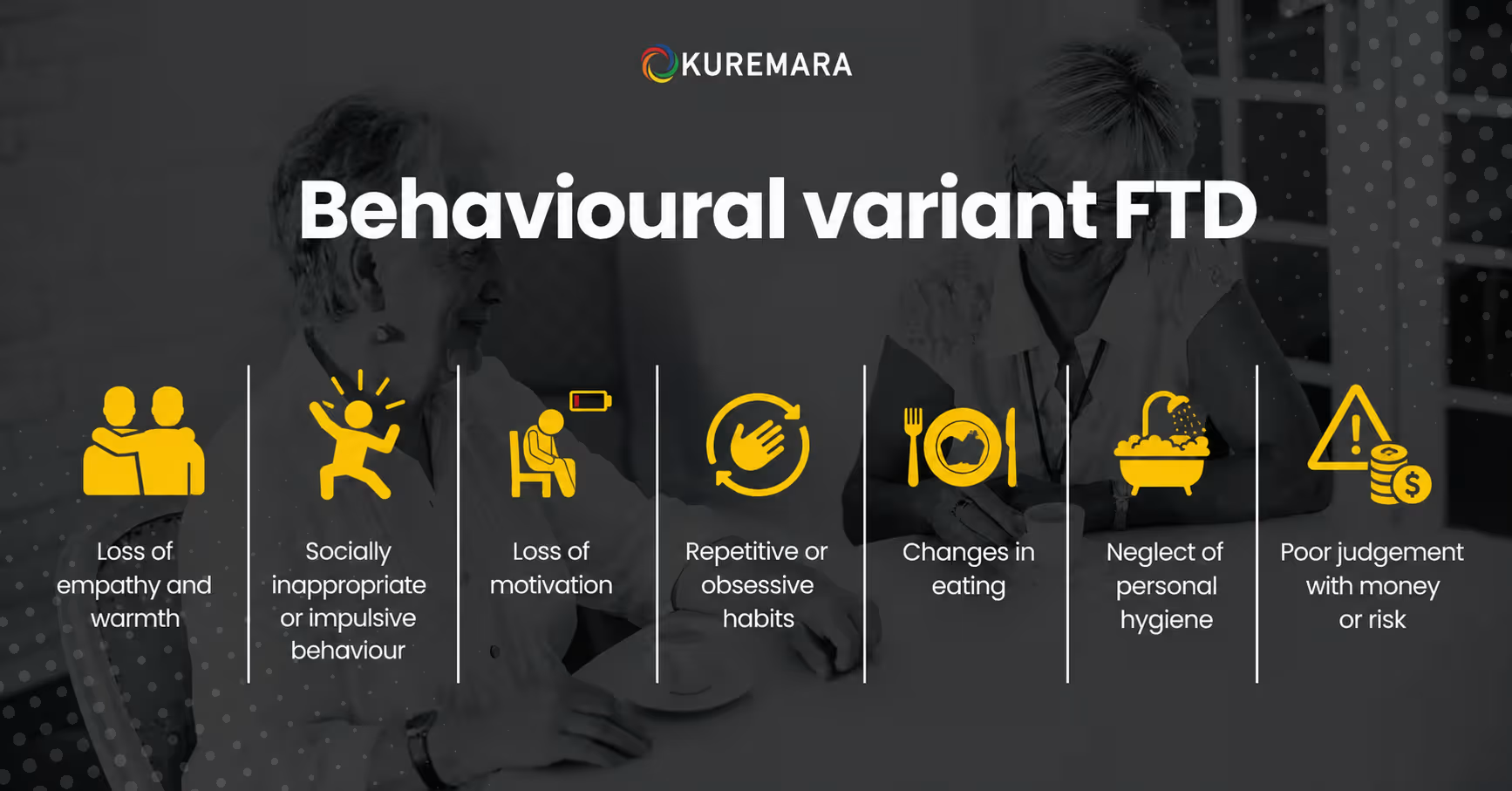
- Loss of empathy and warmth — becoming withdrawn, appearing selfish or unsympathetic, no longer recognising or responding when someone close to them is upset.
- Socially inappropriate or impulsive behaviour — losing inhibitions, making tactless or insensitive comments, acting without regard for consequences.
- Loss of motivation — a growing apathy that can look strikingly like depression, with the person losing interest in hobbies, work, and the people around them.
- Repetitive or obsessive habits — rigid routines, compulsive actions, or fixed rituals that weren’t there before.
- Changes in eating — overeating, a new craving for sweet foods, or other shifts in appetite and diet.
- Neglect of personal hygiene — a previously fastidious person no longer seems to notice or care.
- Poor judgement with money or risk — difficulty planning and organising that often shows up first at work or in the handling of finances.
Read as a list, these are recognisable as symptoms. Lived through in real time, one at a time, over months, they are almost never read that way. They look like a person changing for reasons a family will strain to explain.
2. Language-led FTD (primary progressive aphasia)
In other people, the first casualty is language rather than behaviour. Grouped under the term primary progressive aphasia, these forms include one variant in which speech itself becomes effortful, the person speaks slowly, struggles to make the right sounds, or gets words in the wrong order, and another, sometimes called semantic dementia, in which people gradually lose the meaning of words and struggle to recognise familiar objects or people. Alzheimer’s Research UK describes how someone might forget what everyday objects are for, no longer grasping that a kettle boils water or a remote controls the television. Many people with a language-led form eventually develop behavioural changes too, as the disease spreads.
The “It’s Just Stress” Trap: Why the Diagnosis Comes So Late
Here is the heart of the problem, and the reason this article exists. The behaviours that FTD produces are almost perfectly designed to be mistaken for something else.
The Alzheimer’s Society puts it plainly: symptoms such as risk-taking, loss of inhibitions, or obsessive behaviour can look more like a person going through a difficult or emotionally-challenging time than a medical illness. Even when the changes are recognised as symptoms of something, they are commonly attributed to depression, and sometimes to conditions such as obsessive-compulsive disorder or a psychotic illness. And because the person is often under 65, doctors may simply not expect to see dementia in someone so young.
Two factors make this worse. First, most people with behavioural variant FTD have little or no awareness that anything is wrong. The Alzheimer’s Society notes that these changes are usually first noticed by the people closest to them, while the person themselves rarely feels any need to seek help and may actively refuse it when others suggest it. Second, the standard tests used to screen for dementia largely focus on memory, and memory is exactly the thing FTD tends to spare early on. A person can “pass” a memory test while their life quietly falls apart.
The consequence is measurable, and sobering. Research summarising the diagnostic journey in behavioural variant FTD reports an average delay of around 5 to 6 years from the first symptoms to an accurate diagnosis. In one survey of families, the majority waited more than a year for a diagnosis, over half consulted three or more doctors, and roughly half were initially misdiagnosed (Source: pmc.ncbi.nlb.nih.gov.uk), most often with depression. Those are not lost months; they are lost years, during which families blame themselves, relationships fracture, and no one gets the support they need because no one knows what they are dealing with.
When Should You Think “Could This Be FTD”?
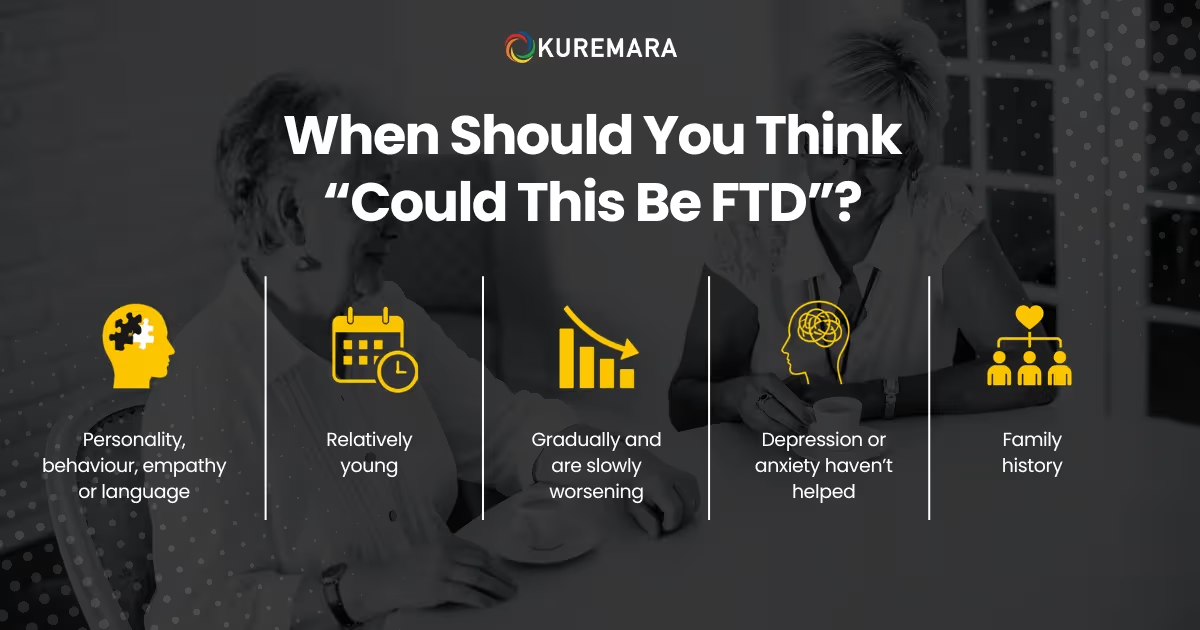
There is no substitute for a specialist assessment, and this article cannot diagnose anyone. But there are patterns that should prompt a conversation with a GP rather than another round of quietly hoping things improve. It may be worth raising the possibility of FTD when:
- The changes are in personality, behaviour, empathy or language, not primarily in day-to-day memory.
- They appear in someone relatively young, often between 45 and 65.
- They have come on gradually and are slowly worsening rather than fluctuating with mood or circumstances.
- The person doesn’t seem aware that anything has changed, while those around them can see it clearly.
- Treatments aimed at depression or anxiety haven’t helped, or the “low mood” is really more like indifference than sadness.
- There is a family history of dementia, FTD, or motor neurone disease in around a third of cases; there is a genetic link, with a parent or sibling affected.
If several of these ring true, it is entirely reasonable to ask a GP directly whether FTD could be explored as a possibility, and to request a referral to a memory clinic, neurologist or old-age psychiatrist. Because someone with FTD is often unaware of their own symptoms, it is especially valuable for a family member who knows them well to attend and give their own account of what they’ve observed. The NHS specifically highlights how helpful this is. Diagnosis usually involves a detailed history, an assessment of thinking and behaviour, blood tests to rule out other causes, and brain scans such as an MRI or CT.
Living With FTD at Home: Where Compassion Meets Practicality
A diagnosis of FTD changes what a family is facing, but it does not change the most important thing: the person is still there, still deserving of dignity, patience and love, even as the illness reshapes how they express themselves. Much of the day-to-day support for FTD happens at home, and there is a great deal that thoughtful care can do to reduce distress on both sides.
Because FTD so often affects behaviour, judgement and impulse rather than memory, the practical challenges can differ from those of other dementias, but the foundation is the same one we explore in our guide to creating a safe and supportive home environment for a person living with dementia: a calm, consistent, familiar setting that lowers anxiety and supports independence for as long as possible. Building on that foundation, families supporting someone with FTD often find a few things especially important.
Consistency and routine matter enormously, because predictability reduces the agitation that unfamiliar situations can trigger. Responding to behaviour rather than reacting to it, asking what a person might be feeling or needing beneath a difficult action, rather than taking it personally, protects the relationship and usually calms the moment. Where impulsive spending, risk-taking, or driving become genuine safety concerns, gentle, practical safeguards put in place early can prevent real harm while preserving as much freedom as possible. And perhaps most importantly, the emotional toll on families is heavy and often invisible; the person providing care needs support just as much as the person receiving it.
That last point is not a footnote. Because FTD frequently arrives in mid-life and changes the very character of a spouse, parent, or partner, it can be one of the loneliest experiences a family goes through. Organisations such as Dementia UK, whose Admiral Nurses specialise in supporting families through complex dementia, and the Alzheimer’s Society offer helplines, guidance, and community for exactly this. No family should be navigating it alone.
How Kuremara Supports Families Facing FTD
At Kuremara, we provide person-centred domiciliary care that allows people living with FTD and other forms of dementia to remain in the comfort and familiarity of their own homes. We understand that FTD is not only a medical diagnosis but a profound emotional one for the person and for everyone who loves them.
Our support is built around the individual rather than the label. That means care shaped by a person’s own history, routines and personality; carefully trained carers who understand how to respond calmly and respectfully to the behavioural changes FTD can bring, without judgement; and genuine respite for family carers, so the people holding everything together get the chance to rest and be supported themselves. Whether a family needs a few hours of visiting care, overnight support, or fuller live-in care as needs grow, we work alongside them to build something that fits their life and adjusts as the condition changes.
If you’re seeing changes in someone you love that don’t quite fit the story you expected, changes in who they seem to be, more than what they can remember, trust that instinct. Speak to a GP, and know that support exists for whatever comes next. If home care could be part of that support, our team is here to talk it through with you, with no pressure and no assumptions, just practical guidance and the reassurance of knowing you don’t have to face it alone.
A Final Word
The cruellest thing about frontotemporal dementia is how easily it hides. It wears the mask of stress, of depression, of a personality simply “changing,” and by the time it is recognised for what it is, years may have passed. But recognition changes everything. It replaces blame with understanding, confusion with a plan, and isolation with support.
If this article does one thing, we hope it plants a single question in the mind of anyone watching a loved one become someone they don’t quite recognise: could this be more than stress? Asking that question and taking it to a doctor is the first step toward the answers, the care, and the compassion that every family facing FTD deserves.
This article is for general information and awareness and is not a substitute for professional medical advice. If you are concerned about symptoms in yourself or someone you care for, please speak to a GP or qualified healthcare professional. Kuremara is a domiciliary care provider supporting individuals and families across the UK.


